











































Designing and Implementing the Adaptive Learning Meeting Cycle: The (re)solve Project Experience in Burkina Faso
Trasi Duarte Consulting (Trasi); Pathfinder International (Angelone, Hounkanrin)
"When implemented in the spirit of continuous improvement and centering the voices of in-country implementers and community stakeholders, RFMs can allow program teams to recognize what is not working, learn from this experience, and adapt to maximize outcome and impact."
Responsive feedback mechanisms (RFMs), such as an adaptive learning meeting (ALM) cycle, can clarify how a programme needs to be fine-tuned and improved to fit into a complex, dynamic system and context. RFMs: engage and centre the voices of the community and local stakeholders in identifying solutions through their professional and lived experiences; are flexible, iterative, and repetitive in nature; and use frequently collected data and dialogue. This article examines how the (re)solve project used responsive feedback to ensure products and services designed and implemented were responsive to the context and preferences of healthcare workers, women, and girls in Burkina Faso.
As detailed at Related Summaries, below, (re)solve was a 5.5-year (2016-2022), 3-country project that combined consumer insights, behavioural economics, human-centred design, and public health to discover what stops women in Bangladesh, Burkina Faso (the focus of this article), and Ethiopia from using modern contraceptive methods, even when they express a desire to avoid pregnancy. The project used an iterative, phased process that drew on multiple social and behavioural theories to design, test, and evaluate (e.g., through a randomised controlled trial (RCT), available at Related Summaries, below) adaptable, scalable, user-responsive solutions for each subpopulation that addressed their context-specific barriers. These solutions were either new products (a digital counseling training app, a board game, and an integrated voice-response system) or new job aids (planning tools and a pregnancy risk assessment tool).
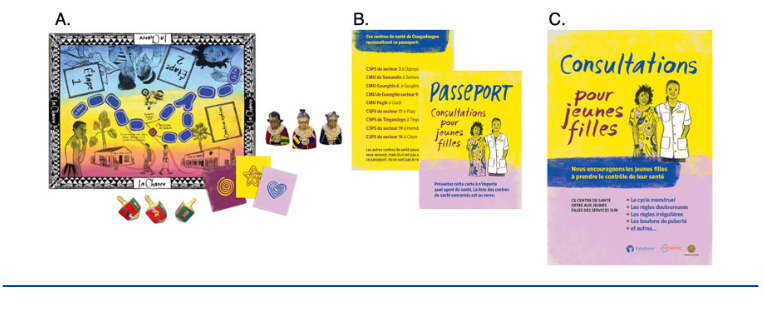
Specifically, from December 2019 to March 2020, the (re)solve project in Burkina Faso implemented the solutions in 16 randomly selected secondary schools, 8 each in Bobo-Dioulasso (Bobo) and Ouagadougou (Ouaga). Organisers conducted orientation sessions on the solutions, their rationale, and the implementation plan with school principals and parent-teacher associations of intervention and control schools (as part of the RCT), as well as with parents of girls in participating schools. Across the 16 participating schools, 32 community-based facilitators implemented the board game ("La Chance") and distributed health "passports" (cueing girls to follow through on their intention to avoid pregnancy by visiting a participating health facility for sexual and reproductive health (SRH) information and services). Posters at participating health facilities publicised services for girls and aimed to normalise their presence at the facility. Two facilitators were assigned to each intervention school, and they conducted 1-2 games per day. A total of 3,120 girls in grades 4ème (grade 9) and 3ème (grade 10) played La Chance between December 2019 and March 2020; facilitators distributed 11,908 passports to girls in this time frame.
As detailed in the article, organisers integrated feedback mechanisms and iterative adaptation into the project framework at 2 key points: (i) user testing during the design and user testing phase and (ii) ALM cycle during the intervention testing phase. Adapted from participatory approaches, the ALM cycle followed a 5-step process for group-based learning and problem-solving using monitoring and observational data that allowed a geographically dispersed project team to learn, be agile, and adapt to real-world implementation challenges. In brief, the steps ("5Ds") involve:
- Discover: Capture data and observations in project monitoring tools; review data; and address logistical and implementation challenges.
- Define: Collate data from all sources; and summarise trends, themes, and challenges.
- Discuss: Interpret data and trends; surface assumptions; and generate and discuss adaptation options and implications.
- Decide: Select and agree on adaptations to implement.
- Deploy: Document and plan adaptations; and implement adaptations.
The first 2 steps took place in Burkina Faso with the implementation team and community-based facilitators; the subsequent 3 steps describe the structure and flow of the virtual, fortnightly meeting with the global team.
During the intervention testing phase, from December 2019 to March 2020, the (re)solve project implemented the solutions in 16 randomly selected secondary schools, 8 each in Bobo-Dioulasso (Bobo) and Ouagadougou (Ouaga). Organisers conducted orientation sessions on the solutions, their rationale, and the implementation plan with school principals and parent-teacher associations of intervention and control schools, as well as with parents of girls in participating schools. Across the 16 participating schools, 32 community-based facilitators implemented the board game ("La Chance") and distributed health "passports" (cuing girls to follow through on their intention to avoid pregnancy by visiting a participating health facility for sexual and reproductive health (SRH) information and services). Two facilitators were assigned to each intervention school, and they conducted 1-2 games per day. A total of 3,120 girls in grades 4ème (grade 9) and 3ème (grade 10) played La Chance between December 2019 and March 2020; facilitators distributed 11,908 passports to girls in this time frame.
By centring the voices of schoolgirls and facilitators when considering the project's adaptation choices, the 5-stage ALM cycle resulted in various context-specific, responsive adaptations. For example, a short-loop adaptation came about when the implementation team learned some girls were bringing their health passports to nonparticipating health facilities. Although they could not provide youth-friendly service provision training to these additional facilities mid-implementation due to the nature of the RCT, the team visited the identified facilities and explained the purpose of the passport and the project to ensure girls would not be turned away and could be referred to participating facilities. There were also long-loop adaptations: recommendations from school administrators, facilitators, or schoolgirls that could not be implemented within the scope and timeline of the project but will be considered for future replication and scale-up efforts.
Per the organiers, the ALM cycle had these additional benefits:
- Acknowledging the contextual expertise of the implementation team and the community-based facilitators at the beginning put them into problem-solving mode. A future area of inquiry could explore whether processes such as these can shift perceptions of ownership, power, and hierarchy within geographically dispersed teams.
- Through its structure, the ALM cycle avoided a skewed focus on analysing the problem and instead shifted the emphasis to action, learning, and adaptation. This shift allowed the implementation and global project teams to collectively recognise when something was not working, learn from it, and move quickly to find a solution.
- The ALM cycle imbued a culture of continuous improvement and efficiency across the team. For example, at each meeting, close attention was paid to which data were being used and which were not. Based on this, some metrics and reflection questions were removed to keep data collection and documentation manageable.
- The team habits and team culture engendered by the ALM cycle had ramifications beyond its intended design and use in Burkina Faso. During the COVID-19 pandemic, for example, the implementation team brought real-time information about curfews and school closures to the meetings, along with an analysis of which aspects of the programme could continue and which ones could not. The evaluation team quickly brainstormed ideas, presented options, and discussed the pros, cons, implications, and feasibility of each option, given the constraints.
In conclusion, RFMs "require careful planning, dedicated time and resources, and careful facilitation of frequent discussions. However, when implemented and nurtured over time, RFMs, like the (re)solve project's ALM cycle, offer a structure and format that can center and elevate the feedback and lived experience of women, girls, and health care workers; engender a commitment to adapt programs to be responsive to this feedback; and build a strong team culture that imbues agile adaptation and problem-solving at all levels."
Global Health: Science and Practice 2023;11(Suppl 2):e2200217. https://doi.org/10.9745/GHSP-D-22-00217. Image credit: Pathfinder International
- Log in to post comments