











































Misinformation: Susceptibility, Spread, and Interventions to Immunize the Public
University of Cambridge
"The spread of misinformation has undermined public-health efforts, from vaccination uptake to public compliance with health-protective behaviors."
In early 2020, the overabundance of COVID-19 information, particularly false and misleading information, led the World Health Organization (WHO) to declare a worldwide "infodemic". Long before this particular pandemic, the spread of misinformation posed a threat to public health. For example, studies find that exposure to misinformation can undermine vaccination uptake. This review provides readers with a conceptual overview of recent literature on misinformation - defined here as false or misleading information masquerading as legitimate news, regardless of intent - along three major theoretical dimensions of the infodemic: susceptibility, spread, and immunisation (boosting psychological immunity to misinformation).
Research question 1: What factors make people susceptible to misinformation? As outlined here, one finding that helps explain why people are susceptible to misinformation is the "illusory truth" effect: Repeated claims are more likely be judged as true than non-repeated (or novel) claims. Although illusory truth can affect everyone, research has noted that some people are still more susceptible to misinformation than others. Individual differences have given rise to two competing overarching theoretical explanations: (i) The "inattention" account, which argues that people are committed to sharing accurate content, but the context of social media simply distracts people from making news-sharing decisions that are based on a preference for accuracy; and (ii) the "identity-protective" or "motivated cognition" account, which argues that the types of commitments that people have to their affinity groups is what leads them to selectively endorse media content that reinforces deeply held political, religious, or social identities. Having discussed emerging evidence for both theories in turn, the paper recommends that we:
- Better integrate accuracy-driven with social, political, and cultural motivations to explain people's susceptibility to misinformation; and
- Define, develop, and validate standardised instruments for assessing general and domain-specific susceptibility to misinformation.
Research question 2: How does misinformation spread in social networks? Researchers have adopted models from epidemiology, such as the susceptible-infected-recovered (SIR) model, to measure and quantify the spread of misinformation in online social networks. A major issue is the existence of echo chambers, in which the flow of information is often systematically biased toward like-minded others. However, studies indicate that "exposure does not equal persuasion (or 'infection')". Based on the analysis of the body of research on "spreading", the paper recommends that future research:
- Outline with greater clarity the conditions under which "exposure" is more or less likely to lead to "infection", including the impact of repeated exposure, the micro-targeting of fake news on social media, contact with superspreaders, the role of echo chambers, and the structure of the social network itself; and
- Provide more accurate population-level estimates of exposure to misinformation by (i) capturing more diverse types of misinformation and (ii) linking exposure to fake news across different kinds of traditional and social media platforms.
Research question 3: Can we inoculate or immunise people against misinformation? Researchers are exploring interventions that are:
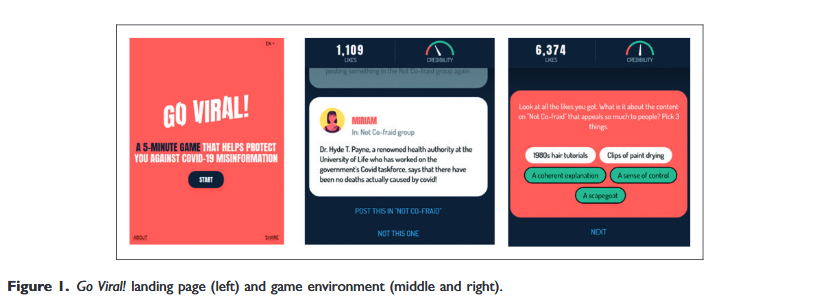
- Prophylactic (preventative - called "prebunking") - The idea is that, by pre-emptively forewarning and exposing people to severely weakened doses of misinformation (coupled with strong refutations), people can cultivate cognitive resistance against future misinformation. For example, research has found that inoculating people against conspiratorial arguments about vaccination before (but not after) exposure to a conspiracy theory effectively raised vaccination intentions. Recent advances in this area include: (i) the move from "narrow-spectrum" or "fact-based" inoculation to "broad-spectrum" or "technique-based" immunisation, with the hope that people become relatively more immune to a whole range of misinformation; and (ii) the application of active versus passive inoculation, wherein people generate their own "antibodies" through, for example, games such as GoViral!", in which players step into the shoes of a misinformation producer.
- Therapeutic (post-exposure - called "debunking") - For example, in one randomised controlled trial, a video debunking several myths about vaccination effectively reduced influential misperceptions, such as the false belief that vaccines cause autism or that they reduce the strength of the natural immune system. Analyses note that the effectiveness of interventions is affected by: (i) the quality of the debunk, (ii) the passing of time, and (iii) prior beliefs and ideologies. Reviews of the literature have indicated that best practice in designing debunking messages involves: (i) leading with the truth, (ii) appealing to scientific consensus and authoritative expert sources, (iii) ensuring that the correction is easily accessible and not more complex than the initial misinformation, (iv) offering a clear explanation of why the misinformation is wrong, and (v) providing a coherent alternative causal explanation. Notably, concerns have been raised about the application of post hoc therapeutic corrections - e.g., the risk of a correction backfiring so that people end up believing more in the myth as a result of the correction.
Recommendations in this third area include:
- Focus on evaluating the relative efficacy of different debunking methods in the field, as well as how debunking (therapeutic) and prebunking (prophylactic) interventions could be combined to maximise their protective properties; and
- Model and evaluate how psychological inoculation methods can spread online and influence real-world sharing behaviour on social media.
In conclusion: "A major challenge for the field moving forward will be clearly defining how misinformation is measured and conceptualized, as well as the need for standardized psychometric instruments that allow for better comparisons of outcomes across studies."
Nature Medicine 28, 460-67 (2022). https://doi.org/10.1038/s41591-022-01713-6. Image credit: Leo Hidalgo via Flickr (CC BY-NC-SA 2.0)
- Log in to post comments