











































A National Network of Public Health and Faith-Based Organizations to Increase Influenza Prevention Among Hard-to-Reach Populations
Emory University (Kiser); University of North Carolina, Greensboro (Lovelace)
"...leveraged their own and others' capacity building resources for community engagement aimed at influenza prevention..."
This report examines a national (United States - US) collaboration to prevent the spread of 2009 H1N1 and seasonal influenza. It highlights how a multilevel, multidirectional, 6-year partnership among the Interfaith Health Program (IHP) at Emory University, the Department of Health and Human Services (DHHS) Partnership Center, the Centers for Disease Control and Prevention (CDC), and the Association of State and Territorial Health Officials (ASTHO) leveraged the capabilities of local public health, health care, and faith-based organisations (FBOs) in 10 communities around the country to increase influenza prevention among hard-to-reach populations.
The report begins by exploring the foundations of the national partnership. From its inception in 1992, IHP, as a national and global intermediary, has worked to eliminate health disparities by convening networks that bridge the public health and FBO sectors. For example, between 2002 and 2007, 78 teams of 400 religious and public health leaders from 24 states participated in 9 CDC-funded and IHP-organised Institutes for Public Health and Faith Collaborations. In 2005, Partnership Center staff attended one of those leadership institutes, where they connected with 10 multisector teams that shared their visions, commitments, and action plans for eliminating health disparities in their communities. Also in 2005, IHP and the CDC convened 6 multisector community networks to develop pilot practices that would increase immunisation rates among minority and vulnerable populations and inform community-level pandemic preparedness.
In 2009, as the World Health Organization (WHO) declared H1N1 to be a pandemic, and with CDC support, the Partnership Center and IHP created "Faith-Based and Public Health Partnerships: Strengthening Community Networks", referred to as "the Influenza Initiative". The goal was to quickly engage organisations that could reach vulnerable, hard-to-reach, and minority populations that were often beyond the reach of traditional public health programmes. It approached this task by fostering networks within and between local communities and among local communities and national entities. To do so, IHP developed a small award process for selecting committed, well-prepared community collaboratives from the cohort of teams that participated in the aforementioned leadership institutes. Selection criteria included being a faith and public health collaborative trusted within the community, having experience with engaging in "ground-up" health promotion and disease prevention with populations experiencing health disparities, and commitment to the goals of the Influenza Initiative. Collaboratives applied, and 9 were selected to form the initial network, with an additional site added in the second year.
The 10 collaboratives focused on capacity building and reach to address barriers to immunisation such as historical mistrust, culture and language issues, and geographic isolation. Each local partnership was led by an organisation with a faith-based identity and mission or a strong outreach programme into diverse faith communities. (Many FBOs are formed and guided by religious principles of serving the economically poor, caring for marginalised populations, and achieving social justice.) For example, Advocate Health Care and its university partner in Chicago, Illinois, US engaged religious leadership in the African American community to understand their mistrust of health care and how health partners could interact with them in respectful, collaborative ways.
Sites chose how to address seasonal influenza prevention (years 2-7) based on their distinctive competencies and the needs of their community. Some addressed upstream barriers to vaccination participation (e.g., mistrust, transportation); some provided education to encourage wider community uptake; and those with clinical capacity provided vaccinations (6 sites).
From 2009 to 2016, IHP, ASTHO, and the Partnership Center worked as intermediaries with these partnerships, fostering information sharing, co-learning, and dissemination of best practices through horizontal and vertical channels. For instance, IHP and ASTHO hosted annual meetings that brought together national partners with representatives from the 10 sites and used a variety of ways to catalyse learning and dialogue among attendees.
IHP designed reporting systems for sites to highlight their unique achievements (e.g., demographic characteristics of populations served, new partnerships, educational and outreach events, success stories, and communications) and to document the number of clinic events and persons vaccinated per site. Several sites conducted focus groups and structured dialogues to explore site-specific issues (immigrant cultural receptivity, preferred preparedness communication methods, etc.).
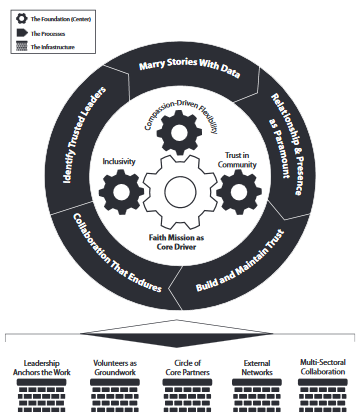
This focus on evaluation is evident in the Model Practices Framework, which IHP, ASTHO, and the 10 sites created during the 2012-2013 project year. As illustrated above and in Figure 1 of the report, the model synthesises the faith-based practices the sites considered essential for reaching vulnerable, at-risk, hard-to-reach, and minority populations. Specifically, it consists of 14 practices organised into a relational model by foundational beliefs (e.g., inclusivity), processes (e.g., marry stories with data), and infrastructure (e.g., circle of core partners).
ASTHO and IHP saw the Model Practices as useful content for a toolkit that could serve as a resource for public health agencies. Designed to be a partnership building tool, "Public Health and Faith Community Partnerships: Model Practices to Increase Influenza Prevention Among Hard-To-Reach Populations" includes information about: the Model Practices, FBOs and the religious landscape of the US, potential faith-based partners around health issues in the public sphere, and guidance on separation of church and state. Partners presented the toolkit content at national conferences, and ASTHO and IHP jointly hosted live and recorded webinars featuring the 10 sites and the Model Practices toolkit content.
Throughout the years, the initiative faced 2 challenges pertinent to national, multilocal, faith, and community-based efforts. The first was the unanticipated misalignment between national and local policies for vaccine dispensing. The second was how one site, a state health department, encountered and responded to the parameters associated with separation of church and state. The report looks at how these challenges were overcome. Among the lessons learned: the need for public health to have strong, multisectoral relationships, the need to understand the capacities of partners, and the importance of clear cross-agency communication.
Based on the evaluation data and reflections by national and local partners, recommendations are offered in the report to assist others in undertaking such a national partnership endeavor. In brief, they include:
- Engage trusted local networks that share commitments to eliminate health disparities.
- Use a framework of strengths and assets.
- Provide a safe and supportive multilocal, multilevel learning community. (For example, throughout the project, a positive frame of strengths and assets was used for progress reports, presentation templates, conference calls, webinars, success stories, and meeting processes.)
American Journal of Public Health (AJPH). 2019;109:371-77. doi:10.2105/AJPH.2018.304826
- Log in to post comments