











































Promoting Adherence to Influenza Vaccination Recommendations in Pediatric Practice
Nemours Children's Hospital (Werk, Cadilla, FranciosiWerk, Cadilla, FranciosiDiaz); Thomas Jefferson University (Diaz); Nemours Children's Health System (Hossain); University of Delaware (Hossain)
"Identifying caregiver motivations and barriers to having their children receive the annual influenza vaccine will be crucial to improving vaccination rates."
In the United States (US), nonadherence to seasonal influenza vaccination guidelines for children and adolescents is common. Although most influenza vaccination recommendations remain consistent each year, with the development of new products and evidence, some are revised. Several strategies have been deployed to promote clinicians' clinical knowledge. A cluster randomised control trial design was used in this quality improvement study to test the effects of 2 interventions on vaccination guidelines adherence with the hope of improving vaccination rates.
The trial involved 11 primary care practices (PRACTICE) that provided care for 11,293 individual children and adolescents in a multistate children's health care system from September 2015 through April 2016. Thirteen clinicians from 11 PRACTICE sites enrolled in the study via an online portal and their sites randomly assigned an intervention arm: No intervention [Control], computerised clinical decision support system [CCDSS], web-based training [WBT], or CCDSS and WBT [both].
A prompt in the electronic health record alerted the primary care clinician to provide an influenza vaccination when a patient 6 months or older who had no record of seasonal influenza vaccination was seen during an office visit at a PRACTICE in the CCDSS arm. The CCDSS included a best-practice alert consistent with the Five Rights Model: (1) "what" (information): reasoning for seasonal influenza vaccination requirement; (2) "who" (recipient): patient; (3) "how" (intervention type): based on age and history, a dosage schedule was suggested; (4) "where" (information delivery channel): links facilitated order entry, documentation of parent refusal, or documentation that vaccine was administered elsewhere; and (5) "when" (in the workflow): the CCDSS was launched when study clinicians opened a patient's office encounter documentation if eligible for influenza vaccine. At subsequent office visits, an electronic prompt alerted the clinician to patients requiring a second dose. Drug-allergy interaction alert would alert as well for those patients with an egg allergy.
Study clinicians receiving WBT were provided links via electronic communications to a 10-minute primer on influenza vaccination recommendations and completed a brief exercise.
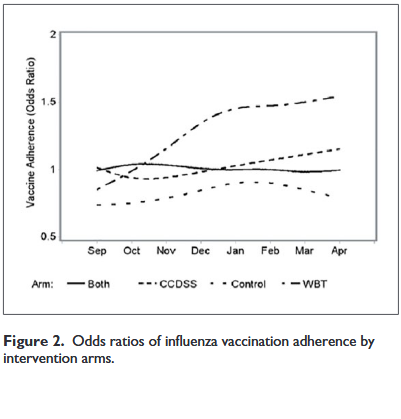
During the study, 55.8% of children and adolescents received influenza vaccination, which improved modestly during the study period compared with the prior influenza season (P = .009). Actual adherence to recommendations, including dosing, timeliness, and avoidance of missed opportunities, was 46.4% of patients cared for by the PRACTICE. The WBT was most effective in promoting adherence with vaccination recommendations, with an estimated average odds ratio (OR) = 1.26, P < .05, to compare between preintervention and intervention periods. Over the influenza season, there was a significantly increasing trend in OR in the WBT arm (P < .05).
Each clinician received a monthly run chart of the rate of vaccination by month for the previous months from October 2015 to March 2016 and list of missed opportunities. Each clinician completed an online progress report at 2-month intervals. Among those in the CCDSS arm, they reported the CCDSS primed mindfulness around vaccination (particularly for those patients requiring a second dose). However, some complained of best-practice alert fatigue. A strategy tested in the WBT arm was to print a copy of the provided algorithm for vaccination and to post it in a visible place. Other strategies included printing a daily patient roster that highlighted patients who would need influenza vaccination and engaging staff to identify eligible patients. Clinicians proposed future process improvements such as adding a message to families to "inquire about influenza vaccination" to the automated telephone appointment reminder. Among those in the Control or WBT arms, clinicians advised developing various electronic prompts, including a best-practice alert.
After discussing the nuances of the findings, the researchers conclude that web-based training at the start of influenza season with monthly reports of adherence can improve correct dose and timing of influenza vaccination with modest impact on overall vaccination rate. However, improvements in influenza vaccination rates may require system changes to work flow, such as moving vaccination out of physician offices into schools or other venues where children and teens assemble. "Providing the appropriate vaccine with correct dose and timing to each child appears problematic in our present system."
Journal of Primary Care & Community Health 10(12):215013271985306, June 2019. DOI: 10.1177/2150132719853061.
- Log in to post comments