











































SBCC Summit 2016 CommTalk: Planning and Budgeting for SBCC Programming
He explains that it could be that SBCC practitioners have not really done enough to show service delivery organisations how they can attain or increase demand or improve coverage through SBCC, or that they have not been shown the value added by SBCC to their activities.
In response to this, the Tanzania Communication and Development Center (TCDC), with support from the Health Communication Collaborative (HC3), has developed an SBCC planning and budget tool which has the ability to calculate the value added by SBCC activities, and allows service organisations to deliver their services at a reduced cost.
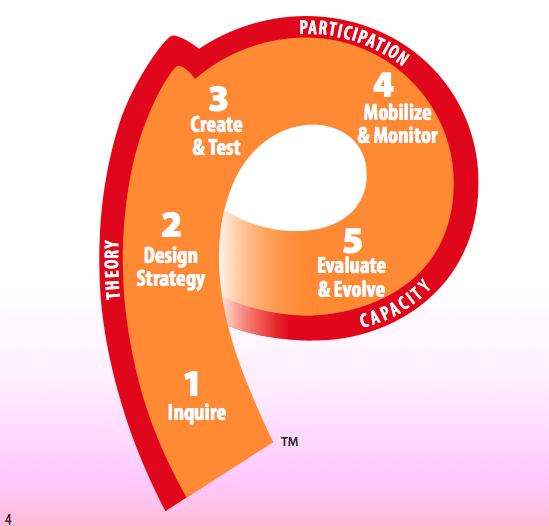
The tool is based on the “P-Process” - a framework designed to guide communication professionals as they develop strategic communication programmes. It includes the following steps: inquire, design, create/test, mobilise/monitor, and evaluate/evolve. The tool allows the user to itemise the cost of each step in the process and to calibrate how SBCC can be used to reduce the cost of overall service delivery. It works on the principal that by stimulating demand through SBCC, service providers can increase coverage and reduce push costs, such as distribution costs, due to increased demand and pull. Deo Ng'Wanansabi explains that TCDC is making this tool available to service delivery organisations in Tanzania through a 3-day course.
Comments

P Process
Deo Wanansabi seems to argue that if P process is followed, demand can be increased for public health services, thereby saving costs by economy of scale. Obviously he has developed tools to develop plans and budget the process. This seems to be a wise approach for convincing the decision makers in simple terms.
Personally I feel the P- process, introduced by the Johns Hopkins Communication Program a long time ago, was a communication strategy planning tool family planning programs that could be used for other public health programs too. However, P-Process introduced initially was not developed keeping in mins SBCC, unless the latest version has evolved to accommodate SBCC approach.
Practically the planning process begins where project ends. In other words, it starts from the evaluation findings of the previous project. In any case the idea is to develop a strategy using the steps in the P-process. Once a strategy is developed it will outline detailed activities that become the basis of budgeting. Is this what Wanansabi is proposing?
To convince the decision makers of the utility of the proposal, nothing less than a A, B, C experiment research model will meet the bill. In such an experiment, as a minimum, three nearly identical areas or communities will be identified. In A, no SBCC activity will be performed, say for three months. In B area, regular promotional or IEC activities may be conducted and in area C, properly planned SBCC program is implemented. In all situation outcome indicators will be same, and their measurement process be also same. I need not dwell on it as local experts know these processes. A thorough evaluation of the project can provide reasonable evidence if and why change occurred, if any.
I realize even if expertise is available to conduct quasi-experiment, funds may be difficult to find. In such a case simply clinic records can be obtained and analyzed.
I have made many assumptions in my argument. If these were wrong, please discard my comments.
- Log in to post comments