











































Using Marketing Science to Understand Contraceptive Demand in High-Fertility Niger
Johns Hopkins School of Public Health (Dalglish); Camber Collective (Vandermark, Neighbor); Université de Genève, and Institut National d'Etudes Démographiques (Rossier); Ministry of Public Health, Niamey, Niger (Kemou)
"Serving subgroups of women based on needs, values, and underlying beliefs may help more effectively drive a shift in FP behavior."
Analyses of demand and social marketing have been used in mass communication campaigns on HIV/AIDS and immunisation, among other interventions. Understanding demand-side determinants of family planning (FP) use is particularly critical in countries like Niger, where both fertility levels and the maternal mortality ratio are high. This article provides a case study of a demand analysis of FP in Niger, based on research conducted by Hope Consulting (now part of Camber Collective) with support from the William and Flora Hewlett Foundation and in partnership with the Ministry of Public Health. The article first describes the research methodology and then presents results of the national survey and resulting segmentation of Nigerien women with respect to FP demand. Its objective is to provide strategic recommendations to help policymakers achieve Nigerien national FP goals by informing communication campaigns, product innovation, pricing, and choice of distribution channels.
Some context, based on literature shared in the article: Demand generation interventions (counseling, education activities, financial incentives) have been found to be positively associated with increases in current use of modern contraceptive methods. However, programmatic interventions have often focused on supply-side approaches, leaving social and behaviour change (SBC) campaigns and demand generation as an afterthought. Progress has been made in improving geographic and financial access to FP in many countries; however, preference for large families continues to drive low contraceptive prevalence rates in parts of sub-Saharan Africa. The researchers of the present study contend that "New approaches to FP programming are required, incorporating an understanding of women's needs, attitudes, and desires so as to improve psychosocial access and offer services and information that speak to women's fertility desires and contraceptive preferences."
Data collection was preceded by consultation with local stakeholders and a literature review drawing from a range of disciplines to understand Nigerien women's fertility management context, including social anthropology, behavioural economics, cultural and health psychology, demography, and gender studies, as well as marketing science and the psychology of consumer behaviour. Exploratory qualitative research was conducted in November 2013, focusing on the Nigerien sociocultural and FP context and including focus group discussions, in-depth interviews with FP providers, and direct observation of FP consultations with urban, peri-urban, and rural women in and outside Niamey, Tahoua, and Zinder. These findings were used to inform the design of a representative survey of 2,004 women of reproductive age (15-49 years) on women's FP knowledge, attitudes, needs, and behaviours. The survey was administered in April-May 2014.
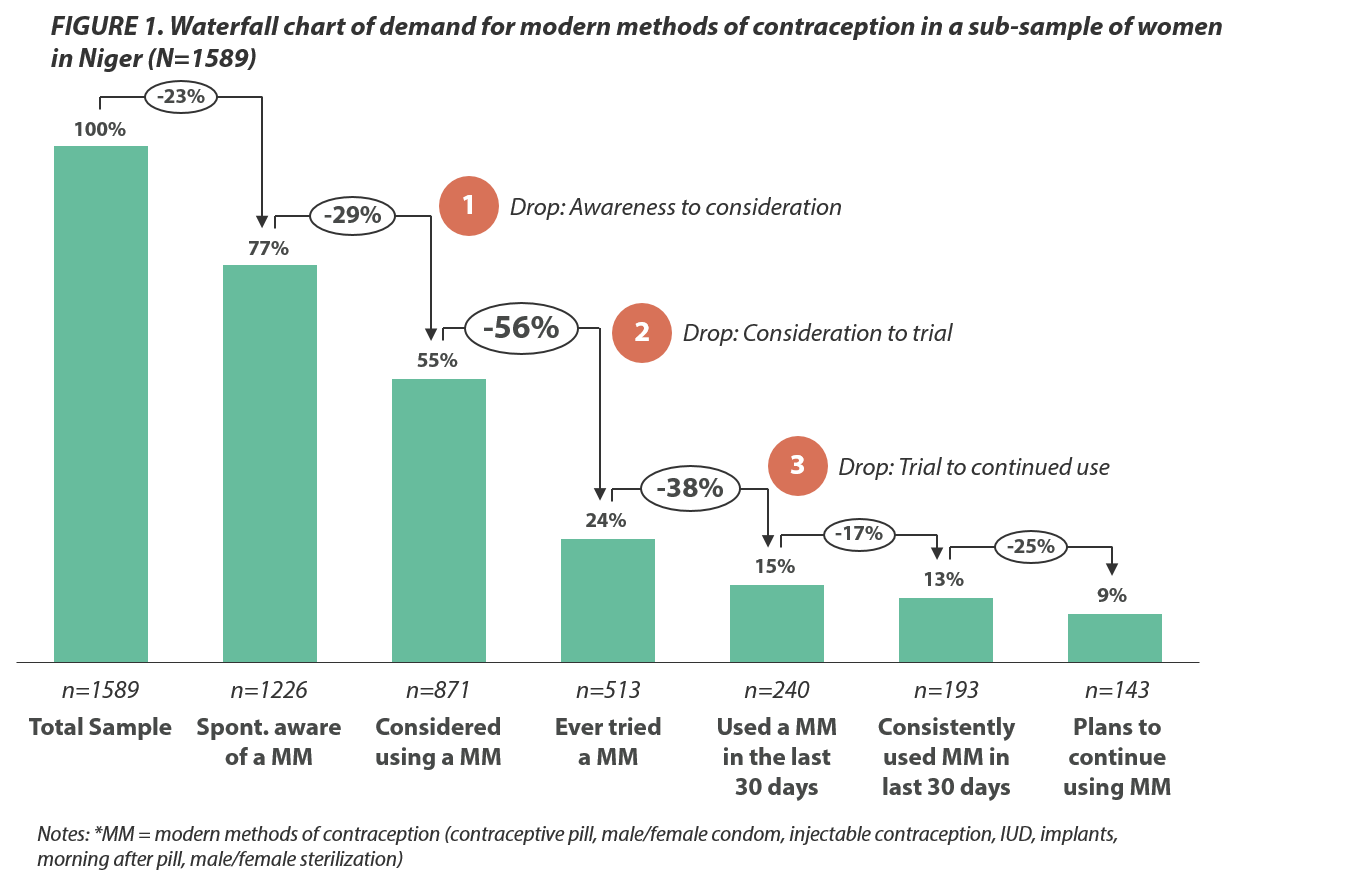
After removing women who were not fertile, in the subsample of women used for the demand analysis (N = 1,589), FP knowledge was moderately high and similar to the overall sample (77% of women could spontaneously name at least one modern method - "MM"). However, 29% of women who were aware of MMs said they did not consider using any MM. Among those who had considered using one, only 44% said they had ever tried one. Of those who had tried one, only 62% had used one in the past 30 days. However, among women who had used a MM in the last 30 days (15% of women), large percentages used it consistently and planned to continue use.
The researchers then used latent class analysis to produce a segmentation of women based on their responses. They identified 5 subgroups of women with distinct, internally coherent profiles regarding FP needs, attitudes, and usage patterns, who faced different barriers to adopting or using modern FP:
- Women in Group 1 (16% of the sample) have the highest rate of MM use as well as a high degree of religiosity, perhaps reflecting a need to show they uphold moral values despite being the only group to accept FP for the purposes of limiting births.
- Group 2 women (28%) also tend to be approving of FP; however, they use traditional methodcs (abstinence and lactational amenorrhoea) as well as MMs to meet their demand and trust healthcare workers to get information on FP more than any other group.
- Women in Group 3 (10%) are somewhat less accepting of MMs and much less accepting of limiting births using FP, although they accept spacing. They are the greatest users of traditional methods of FP in the sample.
- Women in Group 4 (19%) are much less accepting of MMs compared to the other subgroups, and they are most concerned using FP will incur social disapproval.
- Women in Group 5 are by far the least informed about FP, do not use any method, and are highly mistrustful of it.
As data and discussion in the article show, women in the 5 subgroups displayed the following: varying degrees of motivation and autonomy; differences in preferred channels for learning about FP and preferred methods and method characteristics; and different levels of acceptance of or opposition to FP. The first 2 subgroups, Groups 1 and 2, together representing nearly half of the women in the sample, may be relatively well served by traditional approaches to providing FP, as these women are not opposed to modern or traditional methods, are adequately informed, do not fear social stigmatisation for using FP, and proactively reach out to health services. Both of these groups trust healthcare workers and thus can be reached through the healthcare system and served by ensuring steady supplies of MMs and well-informed health workers. However, roughly half of Group 2 women rely heavily on traditional methods. It appears that service delivery and messages are needed to help these women identify and adopt strategies to decrease their exposure to pregnancy.
The results suggest that Groups 3, 4, and 5, making up 57% of the sample, are unlikely to be adequately reached solely via the health system at this time. Women in these subgroups were significantly less accepting of contraception of any kind, and less proactive about seeking out information. These subgroups could benefit from well-designed, sensitive, and ethically informed outreach, SBC campaigns, and community-based interventions. Namely:
- Group 3 women's practices stem from customary beliefs that value birth spacing and women's autonomy, while also promoting high fertility ideals. They may be best reached via appeals to traditional values that are sensitive to and engage with positive images of fertility and large families.
- It is likely that Group 4 would be a difficult group to engage and encourage a change in FP behaviour, as their barriers to FP use are grounded in perceptions of social and religious norms that would take longer to address.
- Messages for Group 5 women - who tend to be young, lack knowledge of FP, and have a low level of pregnancy avoidance needs - could include more general encouragement to learn about the world and consider life choices.
"Taken together, these subgroups of women illustrate the diverse obstacles to promoting psychosocial access to FP in this high-fertility context, including dimensions of knowledge, accessibility, trust, and acceptability."
This demand analysis was presented at a national workshop in November 2014 and has since been used to support FP programming in Niger and neighbouring countries. A toolkit was created for each subgroup with profiles, programmatic guidance, and sample messages (see the Camber Collective website); it has been used by the Nigerien national non-governmental organisation (NGO) Animas Sutura to design improved FP counseling services. A profiling tool containing 12 questions was developed to help service providers quickly categorise women by subgroup during a screening process. In a pilot test in 12 health centres in Maradi, exit surveys showed women receiving counseling that was adapted to their subgroup profile subsequently had higher awareness and use of MMs than women receiving standard counseling. Healthcare workers said the adapted approach to counseling saved them time and improved their ability to connect with clients. The demand analysis is also being used in an SBC communication strategy designed by the international NGO EngenderHealth in Niger, aiming to reach women in Groups 2 and 5 with communication approaches adapted to their profiles. Data from the Niger study have been used by EngenderHealth to design FP messages in Burkina Faso and Togo, focusing on barriers and opportunities to FP use by segment.
Studies in Family Planning, Volume 49, Issue 4. https://doi.org/10.1111/sifp.12078; and email from Sarah Dalglish to The Communication Initiative on June 28 2019.
- Log in to post comments