











































Matching Intent With Intensity: Implementation Research on the Intensity of Health and Nutrition Programs With Women's Self-Help Groups in India
Population Council (Hazra, Das, Ahmad, Singh, Desai); Project Concern International (Chaudhuri); Bihar Rural Livelihoods Promotion Society (Purty); UCL Institute of Global Health (Prost)
"Global evidence syntheses on women's groups have identified significant gaps in our understanding of how these interventions work."
India's self-help groups (SHGs) are voluntary groups of 10-12 adult women who engage in joint savings, credit, and livelihoods activities. In 2017, the Ministry of Rural Development issued an advisory for SHGs to integrate information on food, nutrition, and health with water, sanitation, and hygiene (WASH) into SHG meetings, an approach that is gradually being scaled across several states. This paper aimed to assess the implementation intensity of large SHG-based health and nutrition interventions with rural, low-income women, to inform programme design, delivery, and measurement.
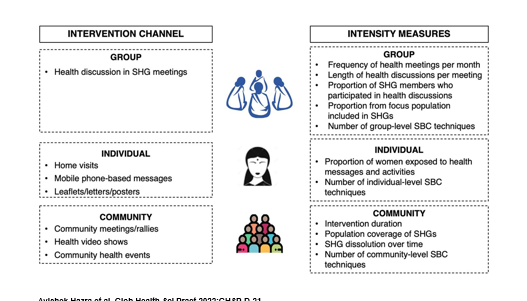
SHG-based health and nutrition interventions centre on the presence of a preexisting group and are premised on women learning new information and skills related to health and nutrition. The population coverage and active functioning of groups influence the community-level intensity of the intervention, supplemented by activities that extend beyond group meetings to reach individuals and community members. Social and behaviour change (SBC) techniques employed by interventions with SHGs include individual-level activities such as information dissemination, as well as group and community-level efforts to address underlying determinants of health, such as building social networks for advocacy. The image above presents 3 main components analysed in this paper: (i) group discussions in SHG meetings (where only SHG members can participate), (ii) individual home visits by SHG members to meet women and family members, and (iii) other community-level events outside of SHG meetings where anyone (SHG members as well as nonmembers) can participate.
The researchers based their analysis on 8 experimental/quasi-experimental studies that included both household surveys and process evaluations of SHGs in 2 Indian states - Uttar Pradesh and Bihar - that discussed health issues for approximately 30 minutes per month in group meetings, with wide variation in member participation across interventions. The most common SBC techniques used were to increase individual knowledge and build social networks. Home visits that aimed to reach women with health information outside of group meetings reached between 30%-40% of households with a group member. Pregnant and breastfeeding women's participation in community events varied across interventions; overall, participation was generally low (less than 25% of women). Most interventions were implemented for at least 1 year, suggesting an intent to achieve health and nutrition outcomes through sustained contact with members, but data from 2 studies indicate that between a quarter and a third of groups dissolved over the intervention period.
As reported here, most of these challenges noted in the reviewed are specific to SHG-based "layering", which is premised on a preexisting, well-functioning, and wide-reaching network of SHGs to deliver information and impart skills. SHGs' primary focus and meeting purpose are financial transactions; as a result, studies report that facilitators had difficulties ensuring that sufficient time was available to discuss health and nutrition. Limited participation or discussions may also reflect a mismatch between member characteristics and choice of discussion topics.
Study implications include, for example:
- Policymakers can explore a range of approaches to address health through working with groups, ranging from information dissemination to community mobilisation. However, they should consider women's health priorities, time availability to participate in intervention activities, and the intensity required to improve health outcomes.
- Where SHGs are not primarily composed of concerned women (i.e., pregnant women or new mothers), home visits or community events are the primary modes for reaching these women. Community mobilisation interventions implemented at scale in India indicate the possibility of inviting other concerned women in the community to SHG meetings, which may improve participation in meetings as well.
- Implementers and researchers should monitor, evaluate, and report implementation intensity of layered interventions, including group meetings, individual visits, and community-based events.
In conclusion: "Interventions that aim to capitalize on existing networks of financial women's groups...will need to have an implementation intensity that matches the ambition of their health objectives: substantial changes in behavioral or mortality outcomes are unlikely to be achieved with relatively light intensity. Interventions that require sustained interactions with members to achieve health outcomes need to ensure adequate community and individual outreach to supplement group meetings, as well as improved participation through more intensive community mobilization approaches. Evaluations of group-based interventions should report on implementation intensity to support the interpretation of evaluation evidence and to inform further scale-up."
Global Health: Science and Practice April 2022, https://doi.org/10.9745/GHSP-D-21-00383.
- Log in to post comments