











































A Quality Improvement Education Initiative to Increase Adolescent Human Papillomavirus (HPV) Vaccine Completion Rates
SUNY Upstate Medical University
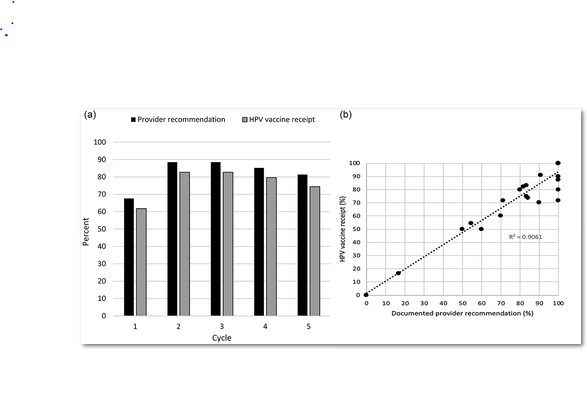
Human papillomavirus (HPV) vaccine uptake is low in the United States (US). The most commonly cited reason for HPV non-vaccination is failure of the provider to recommend the vaccine. Despite vaccine availability and clear recommendations for its use for more than a decade, many providers still describe the vaccine as optional, delay vaccination to a later visit, and/or report parental hesitancy. Motivated by the belief that quality improvement (QI) principles have the potential to change practice, these researchers developed an educational programme designed to enhance QI skills and improve HPV vaccination rates.
Five paediatric practices participated in the initial pilot initiative. Each practice designated one physician provider and one staff member to serve in the role of QI champion for this initiative. In December 2016, the QI champion pairs from each practice attended an off-site education training day that included three 1-hour didactic sessions and a 1-hour-long interactive session, as follows:
- The first didactic session focused on the definition of QI, its process, and commonly used data visualization tools such as value stream maps, impact matrixes, and run charts. Plan-do-study-act (PDSA) cycles were discussed, using several examples.
- The second didactic session, which focused on HPV disease and prevention, modeled strategies for delivering a strong, presumptive vaccine recommendation.
- The third session included an introduction to the American Academy of Pediatrics (AAP)'s web-based data collection tool, QIDA - Quality Improvement Data Aggregator.
- The final session was an interactive discussion about feasible evidence-based systematic interventions, such as use of reminder-recall systems, electronic health record prompts, pre-review of adolescent charts to determine vaccine eligibility, attaching immunisation records to the chart at each visit, and standing orders.
After attending the training session, QI champions shared the QI education materials with all providers and staff in their practice. Their first monthly QI cycle began immediately thereafter. Monthly for 6 months, they performed chart audits, captured data, printed run charts, and developed, implemented, and tracked interventions.
Over the 6 months, mean HPV vaccine completion rates increased (45% to 65%), and missed opportunities for HPV vaccination decreased (45% to 19%).
Participating practices completed a group survey after each monthly team meeting. Survey results indicated that all practices emphasised the role for HPV vaccine in cancer prevention, informed the entire office staff about the QI programme, and provided strategies on how to best support the physician recommendation as a practice-wide philosophy, while also reporting no change in patient visit length. The majority of practices incorporated QI strategies such as bundling HPV vaccine with Tdap and meningococcal vaccines and using personal attestations regarding vaccinating their own children against HPV. Responses from 7 (35%) and 12 (60%) reported no change or an increase, respectively, in provider satisfaction with vaccine communication, and 13 (65%) and 7 (35%) reported no change or an easier operational and clinical flow during the work day, respectively. Reported reasons for parent refusal of HPV vaccine included beliefs that the child is not sexually active, the need for more HPV vaccine information, the desire to wait until the child is older, and concern that the child was not anticipating vaccination at an acute visit.
A second phase included 8 different paediatric practices that received similar training in February 2018. This time, an increase was seen in both HPV vaccine initiation (46% to 61%) and completion (62% to 94%) rates. Surveys indicated that all but one of the practices informed their office staff about the QI programme and provided them with strategies on how to best support the physician recommendation as a practice-wide philosophy. Five of the 8 participating practices used personal attestations regarding vaccinating their own children against HPV, while all 8 practices incorporated the bundling of HPV vaccine and emphasised the role for HPV vaccine in cancer prevention in discussions. Of the 31 surveys with the question answered, 29 (94%) reported a perceived no change or decrease in length of patient visit. Twenty-two (71%) and 8 (26%) reported no change or an increase, respectively, in provider satisfaction with vaccine communication. Similarly, 23 (61%) and 8 (21%) reported no change or easier operational and clinical flow during the work day, respectively.
Key concepts to the success of this programme, which the researchers believe to be generalisable, include focusing on basic QI education, providing strategies to deliver a strong provider vaccine recommendation, reviewing system changes to facilitate vaccination, and engaging all office staff in the effort. On the latter, they suggest that all office staff have the ability to identify, influence and implement changes within a practice and thus should be encouraged to engage and participate in QI initiatives. Practice engagement increases ownership, accountability, and confidence in the model for change.
In conclusion, this study shows that a QI programme that included teaching of essential QI principles and that provided examples of workflow-focused strategies resulted in increases in HPV vaccine series initiation and completion rates among children aged 11-12 years well above the goal of 10%, even when replicated with a second group of practices. One suggestion, per the researchers, is to incorporate communication training into future provider-geared interventions aimed at improving HPV vaccine uptake.
Human Vaccines & Immunotherapeutics, DOI:10.1080/21645515.2019.1627822.
- Log in to post comments