











































Impacts on Breastfeeding Practices of At-Scale Strategies That Combine Intensive Interpersonal Counseling, Mass Media, and Community Mobilization: Results of Cluster-Randomized Program Evaluations in Bangladesh and Viet Nam
International Food Policy Research Institute, or IFPRI (Menon, Nguyen, Saha, Khaled, Kennedy, Ruel, Rawat); Alive & Thrive, FHI360 (Tran, Sanghvi, Hajeebhoy, Baker); Save the Children (Alayon); BRAC (Afsana, Haque); University of South Carolina (Frongillo)
"Combining interpersonal counseling of mothers on optimal breastfeeding practices with a mass media campaign is more effective than a mass media campaign alone, suggesting that using multiple platforms and interventions to improve breastfeeding practices leads to greater improvements in practices than using one strategy alone."
This paper reports on findings from cluster-randomised impact evaluations of Alive & Thrive (A&T) programmes (2009-2014) in Bangladesh and Viet Nam, aimed to improve breastfeeding practices through intensified interpersonal counseling (IPC), mass media (MM), and community mobilisation (CM) - intervention components delivered at scale in the context of policy advocacy (PA). This study evaluated the population-level impact of intensified IPC, MM, CM, and PA (intensive) compared to standard nutrition counseling and less intensive MM, CM, and PA (non-intensive) on breastfeeding practices in these 2 countries.
Described in detail elsewhere (see, e.g., Related Summaries, below), the 2 programme models that were evaluated reached large scale through distinct delivery platforms. In brief:
- In Bangladesh, IPC and CM (e.g., community theatre shows) were delivered by the community-based health platform of a large non-governmental organisation (NGO) called BRAC through its network of field officers, community-based frontline workers (FLWs), and volunteers. The MM component consisted of the national broadcast of 7 TV spots on various aspects of IYCF. PA included workshops to share data, engagement of journalists to broaden reporting on IYCF in the media, creation of an IYCF alliance, and programmes to support breastfeeding.
- In Viet Nam, IPC and CM were delivered through a social franchising approach integrated within the facility-based government health system. Referrals, CM, promotional print materials, and TV advertising were used to generate demand for preventive IYCF counseling services. The MM component consisted of a nationally broadcast campaign using TV and the digital space (internet and mobile phone applications); in intensive areas, the MM campaign also included additional out-of-home advertising through billboards and LCD screens. PA at the national and provincial levels targeted the extension of paid maternity leave to 6 months, strengthening of the code of marketing of breast milk substitutes, and improving provincial planning for IYCF and nutrition actions.
Both implementation models used data-driven approaches that were focused on impact and delivery at scale and adapted to implementation conditions and context, requiring the building of partnerships across diverse stakeholders and the strategic use of multiple harmonised communication channels. Mothers and family members needed to buy into benefits of the recommended practices that were of salience to themselves and their families. Mothers needed to feel confident about the feasibility of making changes, and families and mothers needed to perceive that social norms were shifting. The achievement of scale itself was intended to help shift the perception of social norms related to recommended feeding practices.
Though not generated as part of the present investigation, some findings reported in the article help indicate the scale of the programmes:
- In Bangladesh, between December 2011 and February 2014, BRAC conducted almost 2.2 million home visits to mothers of children 0-5.9 months. This required training more than 11,000 FLWs and supervisors in BRAC alone.
- In Viet Nam, approximately 800,000 children under 2 years of age lived in 15 of the country's 63 provinces where A&T franchises were first established; between January 2012 and December 2014, there were 1.1 million counseling contacts with mothers of infants 0-5.9 months of age at these franchises. Reaching this number of contacts required overcoming caregivers' lack of experience in seeking preventive counseling and required community outreach and TV advertising to generate demand.
- These large numbers of contacts were further enhanced with the addition of national MM campaigns to reach an estimated 8.5 million mothers of children below 2 years in Bangladesh, and over 2 million mothers in Viet Nam. In addition, the media campaigns reached fathers, grandmothers, community leaders, physicians, village doctors, NGO workers, government FLWs, and policymakers.
- In each country, national and provincial or regional advocacy led to greater awareness of IYCF practices in communities and an improved enabling environment that supported investments in scaled-up programmes and helped push the boundaries of scale even further.
The major components of the interventions started at the same time in all intervention areas in both Bangladesh and Viet Nam; with the endline survey in 2014, the total duration of implementation of the full intensive package of interventions was about 3 years in both countries. (Table 1 in the article describes the interventions and the differences between the intensive and non-intensive packages.)
The primary outcome of the analysis presented in this paper is exclusive breast feeding (EBF) in the previous 24 hours, defined as the proportion of mothers of infants 0-5.9 months of age who fed only breast milk (based on a previous-day recall of all foods and liquids). A key secondary outcome is early initiation of breastfeeding (EIBF), defined as the proportion of infants who were reported by mothers to have been put to the breast within 1 hour of birth. Other related breastfeeding behaviours were also measured.
A cluster-randomised evaluation design was employed in each country. For the evaluation sample, 20 sub-districts in Bangladesh and 40 communes in Viet Nam were randomised to either the intensive or the non-intensive group. Cross-sectional surveys were conducted among households with children 0-5.9 months of age before the interventions started (2010) and 4 years later (2014). Difference-in-differences estimates (DDEs) of impact were calculated, adjusting for clustering.
In both countries, the researchers found significantly positive population-level impacts on breastfeeding practices, including higher rates of EBF and EIBF, and lower use of prelacteal feeding and bottle feeding, in areas that received the intensive package compared to areas that received the non-intensive package. In brief:
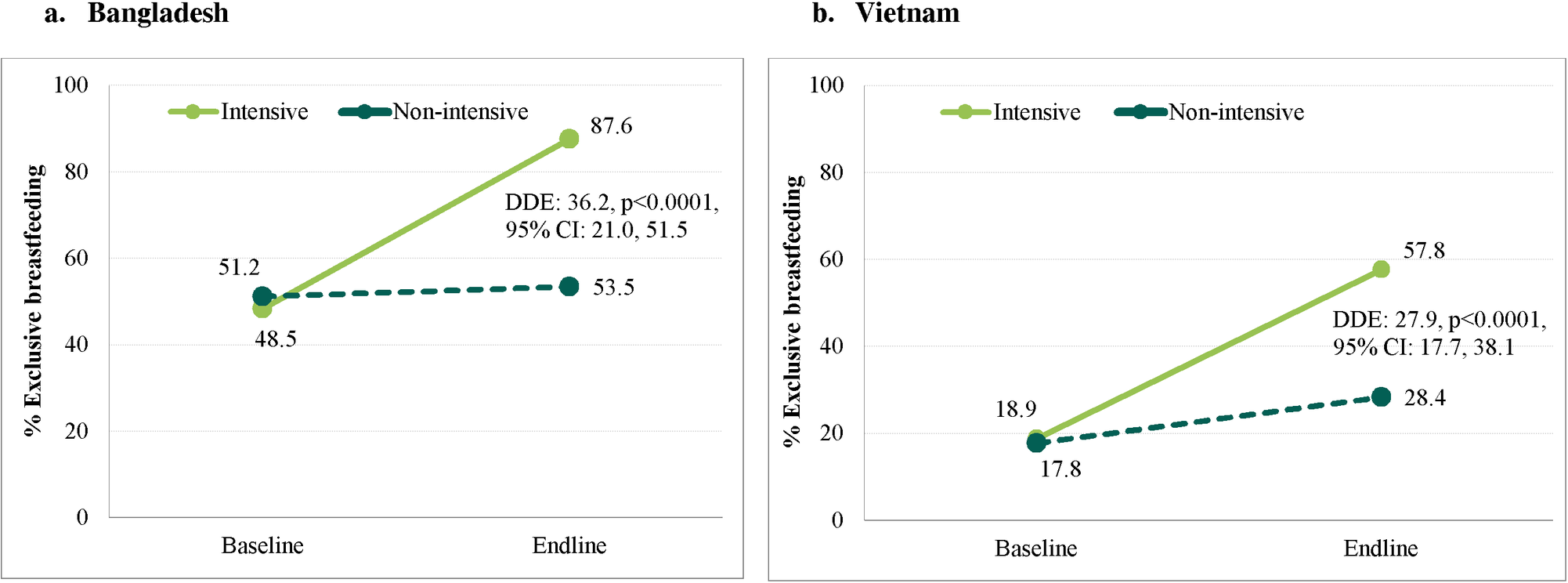
- In Bangladesh, where intensified IPC was delivered through repeated home visits at critical ages combined with CM, improvements were significantly greater in the intensive compared to the non-intensive group for the proportion of women who reported practicing EBF in the previous 24 hours (DDE 36.2 percentage points [pp], 95% confidence interval (CI) 21.0-51.5, p < 0.001; prevalence in intensive group rose from 48.5% to 87.6%) and engaging in EIBF (16.7 pp, 95% CI 2.8-30.6, p = 0.021; 63.7% to 94.2%). The proportion of women practicing EBF at endline was 88% in the intensive group (from a baseline prevalence of 49%).
- In Viet Nam, EBF increases were greater in the intensive group (27.9 pp, 95% CI 17.7-38.1, p < 0.001; 18.9% to 57.8%); EIBF declined (60.0% to 53.2%) in the intensive group, but less than in the non-intensive group (57.4% to 40.6%; DDE 10.0 pp, 95% CI -1.3 to 21.4, p = 0.072). The proportion of women practicing EBF reached 58% (from a low 19% at baseline).
- The impact estimates may underestimate the full potential of such a multipronged intervention because the evaluation lacked a "pure control" area with no MM or national/provincial PA.
Furthermore, in both countries, the breastfeeding-related knowledge of FLWs and volunteers was higher in intensive compared to non-intensive areas. Attendance at a CM session ranged from 12% to 22% in the intensive group in Bangladesh. Maternal exposure to the TV spots was 61%-64% in Bangladesh, and did not differ between groups. Similarly, exposure to TV spots was 70% in Viet Nam, with no statistically significant differences between groups. As expected, awareness and exposure to the social franchise brand was significantly higher among individuals in the intensive than in the non-intensive group.
The researchers contend that the Bangladesh results are generalisable to other programme models that rely on incentivised community volunteers and/or skilled FLWs conducting home-based or community IPC and CM, and suggest that intensifying and strengthening contacts and linking them with MM could have significant benefits. The results for Viet Nam are applicable to other countries where primary health care utilisation is high, MM reach is almost universal, and facility-based platforms can be used to deliver preventive and curative health care. In addition, the results are primarily generalisable to rural areas served by government health services (in countries like Viet Nam) and rural areas in countries like Bangladesh.
The programme appears to have successfully included multiple elements deemed necessary for successful scale-up, including: (1) having a vision for impact on breastfeeding; (2) finding the right combination of interventions and operational contexts; (3) having access to adequate, stable, and flexible financing; (4) actively engaging champions and alliances via PA; (5) using multiple pathways to scaling up: expanding and strengthening capacities (increasing FLWs in Bangladesh and establishing counseling rooms within facilities in Viet Nam); and (6) including adequate learning through the use of data. According to the researchers, looking forward, assessments of the sustainability of these actions at scale will be needed to understand the extent to which these investments led to a sustained legacy focus on infant feeding in the context of the BRAC programme in Bangladesh and the health system in Viet Nam.
In conclusion, using rigorous cluster-randomised evaluation designs, this study "shows that comprehensive behavior change strategies implemented at scale, under real-life conditions, and delivered through outreach-based (Bangladesh) and facility-based (Viet Nam) platforms have strong and significant impacts on breastfeeding practices. Strategies that combine intensive IPC with MM campaigns, CM, and advocacy are more effective than standard counseling with less-intensive accompanying strategies." The researchers conclude that "investments in combined, coordinated, and data-driven strategies, especially those that intensify counseling and are supported by MM, CM, and PA, are recommended for replication in similar contexts and for sustained implementation in Bangladesh and Viet Nam."
PLOS Medicine | DOI:10.1371/journal.pmed.1002159
- Log in to post comments