











































Practice-, Provider-, and Patient-level Interventions to Improve Preventive Care: Development of the P3 Model
Emory University (Bednarczyk, Chamberlain, Mathewson, Omer); Johns Hopkins University (Salmon)
Health promotion and behavioural science theories provide frameworks for understanding human behaviour regarding preventive health care - in particular, why it is often underused. As part of prior and ongoing vaccine acceptance and uptake studies, this team has developed the P3 Model, addressing the practice-, provider-, and patient-level components involved in preventive care for vaccine promotion. In this article, they describe the development of the P3 Model, showing how it addresses gaps left by other health promotion and behaviour models and how it can be adopted and adapted for other preventive care activities. The applicability of the P3 Model is shown through 2 preventive care programme examples: immunisation and colorectal cancer screening.
To situate the P3 Model, the researchers summarise - and describe limitations of - the following commonly used theoretical models:
- The Health Belief Model (HBM) focuses on an individual's perceptions of susceptibility to and severity of disease, along with perceived barriers and self-efficacy related to using the preventive service. The HBM includes modifying factors (e.g., sociodemographics, knowledge) that can impact these beliefs and perceptions, and cues to action (e.g., provider recommendation) that serve to advance acceptance of the preventive service. However, say the researchers, the delivery of these cues to action may be ambiguous; for example, in the case of human papillomavirus (HPV) vaccination, healthcare encounter recordings have documented providers not recommending HPV vaccination with the same directness and emphasis as for other routinely recommended adolescent vaccines.
- Compared to the HBM, the Theory of Planned Behavior (TPB) incorporates and attempts to address a wider variety of underlying beliefs that may affect attitudes, subjective norms, and perceived behavioural control - for instance, it incorporates the concept of control over the decision to undertake the action. However, say the researchers, the TPB may share with HBM the limitation that it is focused on individual patients' attitudes, beliefs, and perceptions, and it does not fully incorporate external influences (broader components of the healthcare system).
- Models that focus on the Shared-Decision Making (SDM) process look at the point in time for the conversation between the patient and healthcare provider without addressing the broader environment, including other communication within the healthcare practice (e.g., intra-practice staff communication). Also, while treatment-based discussions may require a more collaborative SDM approach, SDM-based communication may not be as applicable for routine preventive services.
- The Social Ecological Model (SEM) highlights how individual health decisions exist within an ever-widening sphere of influence - including individual, interpersonal, organisation, community, and policy levels. However, in its attempt to be comprehensive, the SEM poses some issues in terms of clear adaptation for use, implementation, and analysis, say the researchers.
- Social Cognitive Theory (SCT) posits that people learn from one another via observation, imitation, and modeling. However, similar to the limitations described with regard to the HBM and TPB, the researchers explain, there is no clear role in SCT for the physician encounter with the patient.
- The Systems Model of Clinical Preventive Care identifies multiple factors that act on the patient and provider concomitantly. It provides a framework for accounting for this complex web of interactions and factors, offering a set of considerations for developing, implementing, and evaluating preventive care interventions. However, according to the researchers, this model does not fully incorporate healthcare-practice-specific constructs that may impact recommendation or utilisation of preventive care (e.g., appropriate use of electronic medical records and/or immunisation information systems).
Considering the contributions as well as the limitations of these existing theories, the research team conducted a proof of concept study in which they tested the effectiveness of a P3-based intervention to improve antenatal influenza and Tdap vaccination in the obstetric setting. Provider- and patient-level components included vaccine champions, posters, brochures, lapel buttons, provider talking points, an electronic tablet-based educational tutorial for patients, and peer-to-peer education for providers. Despite non-significant differences in vaccine uptake, the majority of physical package components were positively associated with antenatal vaccine receipt, and there were signals that the educational messages were impactful. For example, intervention group women in their third trimester were more likely than similar non-intervention group women to request that their family members consider vaccination to benefit the infant (36% vs. 22%; risk ratio [RR]=1.65, 95% confidence interval [CI]: 1.21, 2.26). Taking the results and feedback obtained from this pilot trial, the team has further developed and fine-tuned this multi-component intervention approach for preventive care services. For example, there are clear areas of focus for practice-level activities across preventive services, including client and provider reminder systems and assessment and feedback activities.
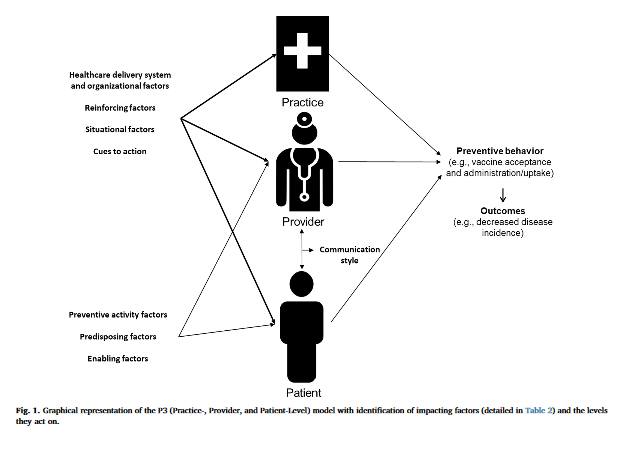
The P3 Model is presented in Figure 1 (see above). The practice-, provider-, and patient-level components are all presented independently, with some impacting factors (e.g., healthcare delivery system and organisation; reinforcing; situational; cues to action) applicable to all 3 levels and some factors applicable to the provider- and patient-levels only (e.g., preventive activity attitudes and beliefs; predisposing and enabling factors). Examples, and related implementation activities or considerations (in the case of predisposing factors), are presented in Table 2 in the article, where the core factors are based on the Systems Model of Clinical Preventive Care.
Based on the layout of the P3 Model, the researchers identify key activities (see Table 3) including:
- Best practices to identify patients needing the preventive service;
- Provider assessment and feedback;
- Use of standing orders (which authorise nurses, pharmacists, and other trained healthcare personnel to administer vaccinations according to a protocol approved by an institution or physician);
- Identification of a prevention/immunisation champion in the practice;
- Consistent preventive activity promotion and messaging across all points of patient contact during the clinical encounter;
- Relevant training for clinic staff; and
- Patient education programmes tailored to the specific population (e.g., use of print, audio-visual, or interactive tablet-based education, alone or in combination).
The researchers contend that the P3 Model allows for inclusion of factors at levels that may not be addressed fully through standard health promotion and behavioural models. For example, healthcare providers may hold beliefs and attitudes that a particular patient may not be at risk of acquiring HPV. With the focus of models such as HBM and TPB on the attitudes and beliefs of the patient themselves, there is a missed opportunity for intervention on the part of healthcare providers' attitudes.
Furthermore, they assert, with the flexibility of components, this model can be implemented across preventive care promotion and adapted to different clinical settings. For example, in community-based settings (e.g., pharmacies and other retail locations), there is still a need for the provider (e.g., the pharmacist) to recommend influenza vaccination and be able to answer patient questions, while also including appropriate practice-level components (e.g., signage indicating that influenza vaccine is available, linkage of the pharmacy to immunisation information systems).
Finally, the P3 Model could be used not only to design but also to evaluate interventions in a way that addresses the multifactorial nature of improving preventive care and also allows interventions to be developed and evaluated in a modular approach to allow future refinement and optimisation of the intervention.
In conclusion: "The practical nature of this model, in terms of understanding key intervention points at each of the levels and developing and conducting evaluation of interventions, makes the P3 Model a flexible and adaptable framework for use across all types of preventive care promotion."
Preventive Medicine Reports, Vol. 11, September 2018, Pages 131-138. https://doi.org/10.1016/j.pmedr.2018.06.009
- Log in to post comments