











































Using an Adaptive, Codesign Approach to Strengthen Clinic-Level Immunisation Services in Khayelitsha, Western Cape Province, South Africa
Australian National University (Timothy); The University of Melbourne (Timothy, Morgan, Kelaher, Danchin); University of Cape Town (Coetzee); JHPIEGO (Morgan); The University of Sydney (Bailie); Murdoch Children's Research Institute (Danchin); The Royal Children's Hospital (Danchin)
"Co-designed, local-level interventions resulted in improvement in parents'/guardians' knowledge about immunisation, parent engagement and service provider commitment to improvement in immunisation service quality."
As in many low-income and middle-income countries (LMICs), optimal immunisation service delivery remains a challenge in South Africa. This is particularly the case in the large, partially informal townships in the Western Cape Province, where there are significant access issues and frequent migration. This study aimed to improve immunisation service delivery in children under 24 months in Khayelitsha, Western Cape Province using an adaptive, co-design approach - a form of participatory action research (PAR) that shares some similarities with the World Health Organization (WHO) tailoring immunisation programmes (TIP) approach - to assess and improve childhood immunisation service delivery at the clinic level.
Phase 1 of the Khusela Immunisation Study included an initial assessment of barriers and facilitators to immunisation service delivery using surveys, focus groups, key informant interviews, and observation. This assessment, which incorporated service provider and service user perspectives and an audit of clinic data and processes, identified barriers to service delivery that were related to issues with vaccine data quality, concerns about access or practical barriers to immunisation, parent engagement and knowledge, and quality of service. (Phase 1 findings will be published separately.) The present paper describes the second and third phases of the study, which include the co-design of local interventions, implementation, and evaluation.
Specifically, between June 2017 and May 2018, a whole-of-systems approach was used that drew on: (i) implementation research and delivery science (IRDS), which allows for the translation of theoretical knowledge into practical, context-specific and evidence-based approaches; and (ii) experience-based co-design (EBCD), which includes collaboration between providers and users, who together design solutions, facilitated by a third party. These approaches were adapted and applied at 3 clinics in Khayelitsha. A mixed-methods approach for data collection and analysis was used, combining both quantitative and qualitative methods.
Key stakeholders in the initial stages of the co-design process included representatives from WHO South Africa and the Western Cape Department of Health, which supported the project. The project working group consisted of 2 representatives from the City of Cape Town Health and service providers from the 3 clinics. Three focus groups, conducted during the final stages of the intervention development process, consisted of 20 service users (parents/guardians).
Based on the identification by key stakeholders and service providers of barriers to and assessment of childhood immunisation service delivery, 4 interventions were prioritised and developed through the co-design process:
- Weekly interactive 1-hour community radio sessions focused on childhood immunisation that were led by nurses and included listener questions.
- Daily 15-minute nurse-led education sessions conducted in clinic waiting rooms, which included a question-and-answer component.
- Service provider and parent quality checklists facilitated by community care workers in clinic waiting areas that served as a prompt to optimise delivery of all components of the immunisation sessions and/or to gather feedback on immunisation service quality and user experience.
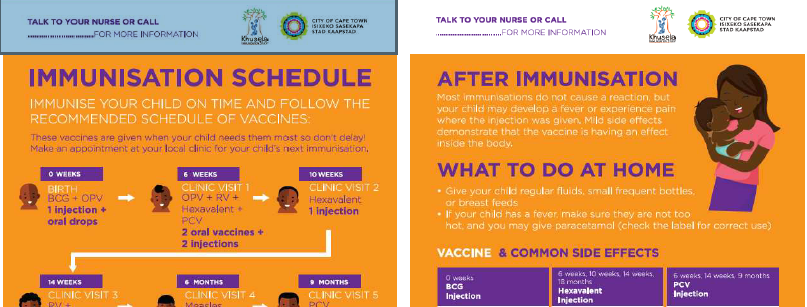
- Health promotion materials - in the form of 4 A2 posters and 4 matching English and isiXhosa A6 postcards for parents to take home (see above for an example) - that were designed by the research team with a local graphical designer based on identified knowledge gaps for parents.
Interventions were implemented for 4-6 months and evaluated using theory-based evaluation tools. Interview and focus group participants comprised 47 Expanded Programme on Immunisation (EPI) service providers, which included 2 representatives from the City of Cape Town Health, 3 health facility/deputy health facility managers, 6 immunisation nurses, 3 pharmacists, 6 clerks, and 26 community care workers. In addition, 369 service users (parents/guardians) participated in surveys (n=352), and 4 focus groups (n=17) and 3 radio staff took part in a focus group.
Selected results:
- Overall, there was no significant change in the number of vaccine doses administered per month before and after intervention implementation. However, an increase was noted in the total number of vaccines administered per month (4% at clinic A, 12% at clinic B, 6% at clinic C).
- Though not statistically significant, there was an increase in parents/guardians agreeing they had sufficient knowledge to make decisions about immunising their child following intervention implementation (pre 57% vs post 75%; difference 18%; p=0.118).
- Significant improvement was noted in parent/guardians reporting they felt comfortable with how they were treated at the clinics (pre 50% vs post 78%; difference 29%; p=0.01).
- Clinic procedures remained mostly the same pre-intervention and post-intervention implementation. However, 58% of the parents/guardians surveyed said they felt waiting times at the clinics were reduced. One community care worker said clinic staff seemed more conscious of following up on clients, with an increase in the number of parents recalled by community care workers and in follow-up reminder phone calls.
- For service providers, overall assessment was very positive for all interventions. Three out of four interventions were well received by parents/guardians, who felt the clinics should continue to support them; the only intervention that had limited reach to parents/guardians was the quality checklists. More specifically, radio sessions and immunisation education materials were deemed most useful by both service providers and caregivers. They valued the simplified presentation of educational information in both. Users valued the 2-way interaction and engagement in the radio sessions. "It was clear that the level of engagement service providers had with each other, and their commitment to improving immunisation services had the biggest impact on whether interventions were successful."
Reflecting on the findings, the researchers note the intersections with TIP work elsewhere (see, e.g., Related Summaries, below), though TIP is usually led by government or national authorities and focuses more on reorganisation of services at the mid or national management levels. That said, the TIP approach "demonstrates the value of participatory problem analysis and co-design to guide responses...Once clinics [in the present study] were aware of the barriers to service delivery, and engaged with the process of intervention development to address these barriers, they became more invested in providing a good quality service."
Key takeaways:
- Rapid experience-based co-design approaches to generate rapid service delivery improvements at the clinic level may prove feasible elsewhere in South Africa and other LMIC settings.
- The approach could be enhanced with a project champion and/or an implementation team to ensure ongoing delivery, assessment, and evaluation of routine immunisation services and expansion of the approach to optimise universal health care (UHC).
- Development of a simplified toolkit and scaled-down approach based on the process used in this study could assist clinics or implementation teams and could enhance the WHO TIP approach for application at the clinic level in LMIC settings.
In conclusion: "Prioritising engagement between service providers and parents/guardians can effectively identify tailored interventions, and be evaluated in a short period to achieve mutual commitment to strengthen childhood immunisation service delivery. This approach provides a framework to guide future local participatory action research for improving childhood immunisation service delivery and other child health services in South Africa and other under-resourced settings."
BMJ Global Health 2021;6:e004004. doi:10.1136/bmjgh-2020-004004.
- Log in to post comments