











































Vaccine Hesitancy: Contemporary Issues and Historical Background
The University of Sydney
"Vaccine hesitancy and anti-vaccine movements have existed since vaccines were first discovered....Although research data have been available in the last decade identifying the causes, consequences, and impacts of vaccination hesitancy, there is still an urgent need to further understand and address public apprehension about vaccines."
An increasing number of individuals view vaccination as unsafe and unnecessary, despite it being recognised as an effective primary public health measure. This review discusses various issues surrounding vaccine hesitancy and the anti-vaccine movement, tracing their history and discussing key drivers across different regions of the world with different socio-economic populations. Having explored the impact of vaccine hesitancy on herd immunity, the review puts forth social, psychological, and public health measures to counter it.
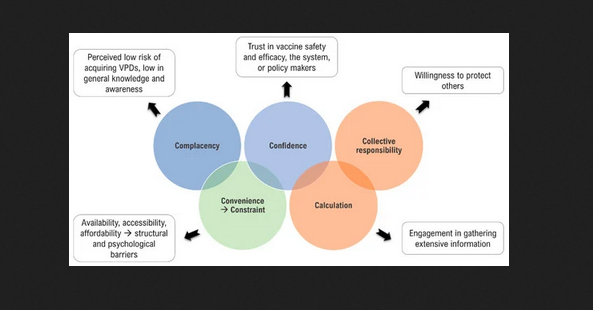
To orient the reader, the paper begins by exploring research that has been conducted to understand the multiple factors influencing an individual's decision to accept or not accept a vaccine. In this regard, the World Health Organization (WHO) Strategic Advisory Group of Experts on Immunization (SAGE) proposed three categories to study these factors: complacency (not viewing diseases as high-risk and vaccination as important), convenience (practical hurdles), and confidence (a lack of trust in vaccine safety and effectiveness), referred to as the 3Cs model. In 2016, a broader nomenclature spanning the dimensions of access, affordability, awareness, acceptance, and activation was suggested for the vaccine uptake determining factors, known as the 5As. Based on both empirical and theoretical research, the 3Cs model was revised in 2018, emphasising the importance of more than just the concept of confidence, which emerged as the 5Cs model: confidence, complacency, constraints (adjustment of the term convenience to now include both structural and psychological barriers), calculation (preference for deliberation), and collective responsibility (communal orientation). (See the image above, which depicts the adjustment of the vaccine hesitancy model from 3Cs to 5Cs.)
As outlined here, skepticism and suspicions about vaccines and the motivations behind their use emerged early, when Edward Jenner developed the first smallpox vaccine in 1796. Numerous anti-vaccination publications emerged in the 1870s and 1880s, and anti-vaccination movements started to appear across Europe. Between 1920 and 1970, new vaccines for tuberculosis, yellow fever, whooping cough, tetanus, and polio were introduced, dramatically lowering childhood mortality. However, this time period and years that followed saw a number of vaccine controversies that challenged public trust in vaccines' efficacy and overall safety, including: the Cutter incident and Simian Virus 40 (related to the polio vaccine); issues around the swine flu vaccine and Guillain-Barré Syndrome (GBS); media coverage of and a documentary on the diphtheria, tetanus, and pertussis (DTP) vaccine; Andrew Wakefield and the measles, mumps, and rubella (MMR) vaccine; and the thiomersal controversy.
Next, the paper looks at drivers of vaccine hesitancy, with a wide range of socio-demographic, attitudinal, and knowledge-based factors being important. Attitudinal factors, such as one's cultural and religious beliefs, the perception of risk or harm, and the behaviours of oneself and others, play critical and interconnected roles in decision making. COVID-19 vaccination has been specifically connected to political affiliation, ideological and partisan factors, information (including mis- and dis-information), and satisfaction with government decision making on other aspects of COVID-19 prevention strategies and/or management. In addition to vaccine hesitancy in the COVID-19 era, topics covered by the review are: heuristics and vaccine hesitancy, concerns regarding vaccine safety and efficacy, the internet and social media influence, and mandatory vaccination and public health policies.
Concerns about vaccine safety and efficacy are most common in high-income countries (HICs), whereas in low- and middle-income countries (LMICs), cultural and religious beliefs, negative historical experiences with foreign medicine and vaccination campaigns, and issues within healthcare systems are more common. For instance, in 2003-2004, a boycott of polio vaccination occurred in five Muslim-majority states of northern Nigeria after religious and political leaders endorsed rumors that the oral polio vaccine was part of an American plot to spread HIV and cause infertility. Factors that are common to both HICs and LMICs include distrust in medical companies and the government, conspiracy theories, and social media misinformation.
Measures to counteract vaccine hesitancy outlined in the review include:
- Public education and communication that is multi-cultural and multi-lingual - "Such communications about vaccine safety and population health benefits of vaccinations must be delivered by individuals who are trusted by the community, for example, high-profile role models, as well as individuals who are able to answer questions and queries in an objective and non-judgmental manner..."
- Behavioural interventions and catalysts for change - "Promoting behavior change to encourage vaccination acceptance and uptake is a complex process that incorporates various social impacts on individual decision making and requires coordinated activity at multiple levels by individuals."
- Importance of political will and leadership - "How governments respond to disease outbreaks in general has a significant impact on public trust in regard to vaccination....They bear an obligation to offer accurate and unbiased health information, and not doing so can lead to increased concerns about vaccination."
- Pivotal input from healthcare providers/clinicians - "Since healthcare workers are the most knowledgeable in the relevant field and are among the first to receive vaccinations, they should be able to speak authoritatively and confidently to their patients about their decision to receive vaccines themselves and encourage their patients and families to also receive the vaccines..."
- Mandatory vaccinations - "...can be ethically justified if the following conditions are met: the threat to public health is grave, the confidence in safety and effectiveness is high, the predicted value/benefit exceeds the alternatives, and the coercion is applied in a proportional manner (e.g., non-compliance penalties or costs are reasonable)..."
In conclusion: "As we slowly emerge from the last two years of COVID-19 and health restrictions, it is even more critical to conduct focused research on vaccine hesitancy to obtain a deeper and more thorough understanding of community dynamics, socio-cultural influences, and indigenous knowledge and beliefs, as well as how criticisms about vaccines and vaccinations; whether valid, false, or perceived to be true; can affect vaccination acceptability, and how to overcome these concerns in a non-judgmental and measured manner."
Vaccines 2022, 10(10), 1595; https://doi.org/10.3390/vaccines10101595.
- Log in to post comments