











































Vaccine Hesitancy in Migrant Communities: A Rapid Review of Latest Evidence
University of Washington School of Public Health (Tankwanchi, Garrison); University of the Witwatersrand (Bowman); Seattle Children's Hospital and University of Washington (Garrison); University of Washington School of Medicine (Larson); London School of Hygiene and Tropical Medicine (Larson); Cochrane South Africa, South African Medical Research Council (Wiysonge); Stellenbosch University (Wiysonge); University of Cape Town (Wiysonge)
"[M]ultiple outbreaks of vaccine-preventable diseases among some immigrant communities in host countries with otherwise high vaccination coverage suggest vaccine hesitancy could be a factor in their health vulnerabilities..."
Grounded in rumours and misinformation about the safety and effectiveness of vaccines, and digitally enabled by the internet and social media, the viral spread of vaccine hesitancy has been associated with diminishing public trust in science and in vaccination in multiple countries. Although vaccination is often required for immigration and refugee resettlement, many immigrant communities experience lower immunisation rates and higher burden of vaccine-preventable diseases than host populations. This rapid review examines evidence of vaccine hesitancy within migrant communities in the context of increased human mobility, anti-immigrant sentiment, and xenophobia.
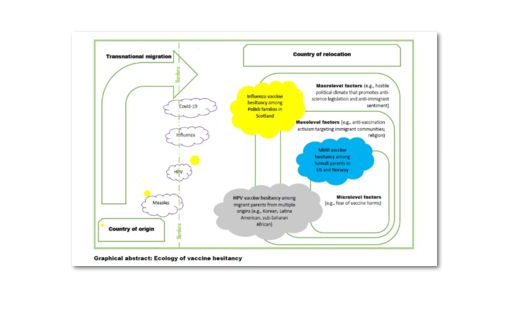
The review reveals evidence of measles vaccine hesitancy in the Somali and Romanian diasporas. For example, although a consistent body of research has shown no causal relationship between the measles-mumps-rubella (MMR) vaccine and autism, misinformation about such a link has permeated clusters of the United States (US)-based Somali immigrant population in Minnesota. There, MMR vaccination compliance among Somali children plummeted from 92% in 2004 to 42% in 2016, leading to a measles outbreak between March and August 2017, with Somali Minnesotans constituting 81% of the cases. And in Sweden, Somali mothers who delayed MMR vaccine due to concern about side effects experienced perceived stigmatisation by Swedish health personnel who ignored their concerns or prejudged their stance on vaccination.
Research has also documented low influenza vaccination uptake rates among United Kingdom (UK)-based Polish immigrant children. Evidence suggests that Polish immigrant parents held many of their health beliefs and vaccination concerns before moving to the UK and continue to be influenced by the Polish diaspora mass media and social media out of Poland, where a highly organised anti-vaccine movement is bolstered by widespread political populism in Eastern Europe associated with anti-science, anti-Western, and anti-immigrant sentiments.
Although African countries have some of the world's highest incidence rates of cervical human papillomavirus (HPV) infection, a study of parental attitudes towards HPV vaccine found widespread reluctance vis-à-vis the vaccine among UK-based immigrant parents from Kenya, Nigeria, South Africa, Zambia, and Zimbabwe. Hesitancy was driven by concerns that approving the HPV vaccine for their daughters was tantamount to granting them a license for promiscuity. Some suspicious parents believed HPV vaccine is a racist biopolitical strategy designed to sterilise Black/African girls for population control purposes. Another example of HPV vaccine hesitancy is among Somali Minnesotan parents and young adults, who reportedly perceived an incompatibility between HPV vaccine uptake and their Muslim faith, which precludes premarital sex. By and large, limited knowledge of both cervical cancer and HPV vaccination, as well as religion-driven social conservatism that hinders open and informed conversation about sexual and reproductive health, are some of the main drivers of HPV vaccine hesitancy among many immigrant families.
Taken together, the identified drivers of vaccine hesitancy in migrant populations can be aggregated in three main analytical categories consistent with the "3Cs" of vaccine hesitancy proposed by the SAGE Working Group on Vaccine Hesitancy: complacency, confidence, and convenience. As suggested here, these Cs interact to cause vaccine hesitancy among migrants through a pathway of social exclusion: Experiences of marginalisation or discrimination in host countries may lead immigrant communities to distrust the health system and health providers, culminating in vaccine hesitancy as an expression of cultural alienation or even an active skepticism of the healthcare practices of the host culture.
Reflecting on the analysis, the researchers suggest that political discourses that fuel prejudice and exclusion of "the other", as well as restrictive policies that prohibit access to universal health coverage to migrant populations, represent as great a barrier to immunisation as does vaccine hesitancy, and perhaps fuel the latter.
In conclusion: "effective strategies to increase and sustain optimal vaccination coverage in migrant populations will be those that combine community-based immunization service delivery tailored to the specific health issues and unmet social needs of a given immigrant community with migrant-friendly health systems and policies that affirm and protect their human rights and dignity..."
Current Opinion in Immunology 2021, 71:62-68; and email from Akhenaten Benjamin Siankam Tankwanchi to The Communication Initiative on August 19 2021. https://doi.org/10.1016/j.coi.2021.05.009.
- Log in to post comments