











































Building and Sustaining Public and Political Commitment to the Value of Vaccination: Recommendations for the Immunization Agenda 2030 (Strategic Priority Area 2)
JSI Research & Training Institute, Inc (Olayinka, Shimp); Johns Hopkins Bloomberg School of Public Health (Sauer, Wonodi); World Health Organization (Menning, Lindstrand); UNICEF (Summers); Gavi, the Vaccine Alliance (Mackay); Dalhousie University (MacDonald); University of the West Indies (Figueroa); freelance consultant, Parliament of Madagascar (Andriamitantsoa); Government of Ghana (Bonsu); Government of India (Haldar)
"To build strong acceptance and demand for vaccination among caregivers and their communities, national governments must be committed to delivery of quality services, building trust and engaging communities to ensure that programs are responsive to the needs and perspectives of all people across the life-course."
Despite being a core component of public health systems worldwide, immunisation services are vulnerable to a range of challenges that threaten continued political, financial, and public support, not least among them the ongoing COVID-19 pandemic. The Immunization Agenda 2030 (IA2030) identifies commitment and demand as critical strategies for achieving and maintaining high immunisation coverage and addressing equity and sustainability challenges. Building on the agenda's collaborative development process, interventions to improve commitment and demand aim to be people centred, partnership based, country owned, and data guided. This paper summarises IA2030's Strategic Priority 2, which describes key challenges to commitment and active uptake of vaccination and provides recommendations to strengthen buy-in at all levels - from community members to global leaders.
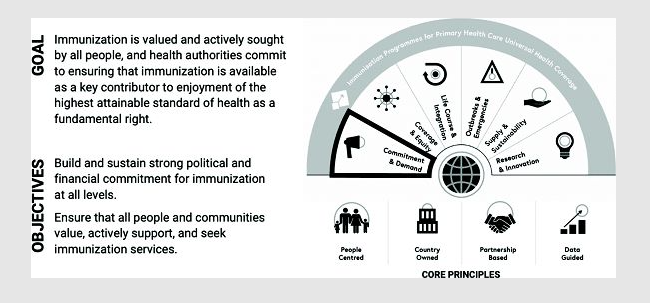
Having outlined key focus areas for commitment and demand (see figure 3), the paper examines the three barriers that will need to be addressed in order to achieve national and subnational immunisation targets by 2030:
- Shifting leadership priorities and resource constraints - Decision makers must balance complex and often competing political priorities with commitments to existing health programmes, while also meeting the needs of their populations and exercising fiscal judgment with donor and domestic resources. This includes managing resource transitions (financial, human, and programmatic) for routine immunisation and disease-specific interventions that have their own life cycles, such as the winding down of the Global Polio Eradication Initiative (GPEI) and COVID-19 vaccination efforts.
- Visibility of disease burden - In contrast to emergency response situations (e.g., COVID-19), many diseases prevented by vaccination are less visible, often thanks to the success of vaccines and vaccination programmes; other vaccines are provided to prevent disease many years in the future. Greater effort may be required to communicate the risk of disease and the value and benefits of vaccination, cultivate stakeholder support, and ensure that immunisation services are easily accessible and appealing to a broad age range.
- Social and behavioural drivers - In some settings, lack of local data on the drivers and facilitators of vaccine uptake - or inadequate gender-responsive community engagement to understand priorities - may impede efforts to design, implement, and evaluate targeted interventions to improve immunisation acceptance and demand.
IA2030 proposes a set of interventions across five interconnected domains to address these barriers: building and sustaining national commitment, supporting subnational leadership and community engagement for immunisation across the life course, ensuring accountability at all levels, promoting acceptance and demand for vaccination, and addressing reluctance to vaccinate. Note that each of the five areas is interconnected, with data cross-cutting all.

For example, in the area of promoting acceptance and demand for vaccination, the authors of this paper recommend the following approaches, among others:
- Engaging communities and civil society in planning and implementing quality services, which can help reinforce social norms to vaccinate and present vaccination as a social contract. Co-development of a programme through evidence-informed social and behaviour change activities can improve knowledge, motivations, and intentions, as well as activate vaccination through reminders, prompts, or primes that better respond to the needs and context of the community.
- Building and sustaining public trust in immunisation, which is essential to ensure community demand. In addition to health workers, trusted civil society organisations, faith-based leaders, and community leaders can play a key role by channeling information on public needs, priorities, and concerns to relevant authorities and programmes and facilitating interactions between communities and service providers.
- Carrying out ongoing media monitoring and listening to individuals and communities, which is important for understanding fears and concerns and addressing people's specific needs. Strategies to monitor rumours, misinformation, and disinformation - both online and in the community - can help inform tailored messages to limit their spread and mitigate hesitancy.
- Recognising the influence of individual and contextual determinants on vaccination behaviours, including how people access information and their motivations. With multimedia information sources readily available, authorities have the means to consider a wide range of channels and trusted spokespeople, communicate proactively and factually, and have robust coordination mechanisms and response plans in place.
- Creating social and political will from the grassroots up that promotes and sustains demand for vaccination and that positions immunisation as a positive, protective care practice for children and adolescents, pregnant women, and older populations.
- Integrating immunisation into education curricula and broader health promotion and literacy strategies.
In conclusion: "People must be at the center of immunization programs....Civil society, community leaders, social networks, caregivers, and individuals all play important roles in vaccination uptake and confidence-building and serve as powerful advocates to exert pressure on decision-makers to improve vaccine availability for all across the life course, including the most vulnerable. As we implement IA2030, countries and partners must be equipped to gather reliable, high-quality data on immunization program status and drivers of community demand, and to employ human-centered design and people-centered approaches that enhance and build on traditional approaches and improve commitment at all levels."
- Log in to post comments