











































Improving Rates of Outpatient Influenza Vaccination Through EHR Portal Messages and Interactive Automated Calls: A Randomized Controlled Trial
Veterans Health Administration (Cutrona); University of Massachusetts Medical School (Cutrona, Barton, Fisher, Mazor); Meyers Primary Care Institute (Golden, Garber); Baystate Medical Center (Goff); Tufts University School of Medicine (Goff); Brown University (Ogarek); Reliant Medical Group (Fisher, Preusse, Sundaresan, Garber)
"This outreach represents a successful brief patient engagement effort."
Despite widespread publicity promoting influenza vaccination, vaccines are underutilised in the United States (US). In 2013, national vaccine coverage for influenza was 41.0%, yet the Healthy People 2020 target was 70%. One of the patient outreach interventions that has been explored to promote influenza (and pneumococcal) vaccination is electronic health record (EHR)-tethered portals. Studies show that patient portals can enhance patient empowerment, improve medication adherence, reduce office visits, increase self-management of disease and disease awareness, encourage the use of preventive medicine, and foster the inclusion of patients in decision-making. In light of those findings, this group of researchers conducted a randomised controlled trial (RCT) using EHR patient portal messages and interactive voice response (IVR) calls to promote influenza vaccine completion, as well as to solicit patient self-reports - e.g., on barriers to vaccination.
The non-blinded RCT was conducted at a large multi-specialty medical group in central Massachusetts, US. The study consisted of portal-based or IVR outreach, beginning November 10 2014. The primary outcome was EHR-documented influenza vaccine administered during the 2014-2015 influenza season. Qualitative interviews with patients, physicians, nurses, and staff informed the development of outreach material.
Using a factorial design, the researchers assigned 20,000 adults with no documented influenza vaccination two months after the start of influenza season (2014-2015) who were already active portal users to one of four study arms:
- Receipt of a portal message promoting influenza vaccines - Characteristics unique to the portal message (as compared to IVR) included access to direct online scheduling of influenza vaccination appointments. Information about the Centers for Disease Control and Prevention (CDC) vaccine website(s) appeared within the body of the message as a hyperlink (conveyed verbally via IVR). Opportunities to report community-administered influenza vaccinations, barrier questions, and targeted information dispelling misconceptions matched the IVR call content. Among these patients, those also overdue for pneumococcal vaccination received outreach with additional messaging encouraging them to speak with their healthcare provider about pneumococcal vaccines, as well as a CDC hyperlink for more information.
- Receipt of IVR call with similar content - Combining speech recognition with branching logic, calls elicited patient self-report of influenza vaccinations completed outside the medical group. For patients reporting no vaccine, calls asked about barriers and responded with brief, targeted education. As with portal messages, information on pneumococcal vaccines was given to eligible, overdue patients.
- Both 1 and 2.
- Neither (usual care).
In addition, the researchers randomised 10,000 non-portal users to receipt of IVR call or usual care.
Among portal users, 14.0% (702) of those receiving both portal messages and calls, 13.4% (669) of message recipients, 12.8% (642) of call recipients, and 11.6% (582) of those with usual care received vaccines. On multivariable analysis of portal users, those receiving portal messages alone (odds ratio (OR) 1.20, 95% confidence interval (CI) 1.06-1.35) or IVR calls alone (OR 1.15 95% CI 1.02-1.30) were more likely than usual care recipients to be vaccinated. Those receiving both messages and calls were also more likely than the usual care group to be vaccinated. Among non-portal users, 8.5% of call recipients and 8.6% of usual care recipients received influenza vaccines. Pneumococcal vaccination rates showed no significant improvement.
In short, the study demonstrated a small but statistically significant improvement in completion of influenza vaccination among portal users receiving a portal message, an IVR call, or both. Adding IVR to portal messages was slightly but not significantly better than messages alone, and IVR calls among non-portal users did not improve vaccination rates. ("IVR alone worked better with portal users than non-portal users, perhaps due to a higher level of healthcare engagement among portal users....[A]n IVR call acting as reminder and facilitator (e.g., list of upcoming clinics) might have adequately addressed barriers for a higher percentage of people in this population.")
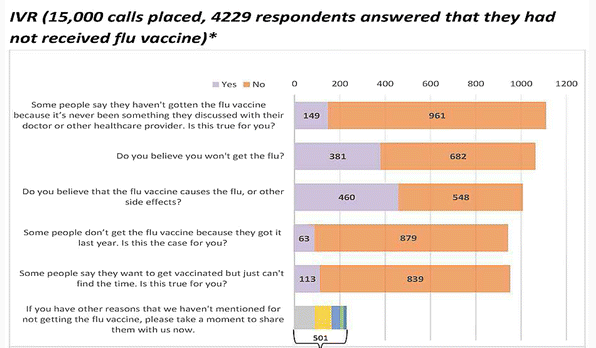
The researchers also gained insight into barriers for over 1,000 unvaccinated patients (see Figure 2 in the paper). For example, more than half of those responding to the portal barrier questions had not discussed the vaccine with a healthcare provider. Commonly cited barriers included fear of vaccine side effects and the belief that they would not get the flu. The researchers assert that provider discussion and educational materials have the potential to address these barriers.
Among the ideas for further research offered here is exploring ways to improve engagement through adjustments in outreach timing or message content.
Based on this study, the medical group with which these researchers are affiliated plans to continue yearly portal outreach for influenza vaccination. They have adapted the messages in response to physician requests, specifically aiming to reach paediatric populations at high risk for influenza. In conclusion, the "intervention's small effect size is matched with considerable reach and sustainability, increasing its potential impact....Through existing portal functions embedded within a widely implemented EHR vendor, [the]...intervention design lends itself to sustained use across diverse settings and with limited resource expenditure."
Journal of General Internal Medicine, May 2018, Volume 33, Issue 5, pp 659-67.
- Log in to post comments