











































Effect of Automated Immunization Registry-Based Telephonic Interventions on Adult Vaccination Rates in Community Pharmacies: A Randomized Controlled Trial
National Quality Forum (Stolpe); Harvard Medical School, Harvard T.H. Chan School of Public Health, and Brigham and Women's Hospital (Choudhry)
There has been a significant increase in the number of patients who receive their vaccines in community pharmacies in the United States (US). Pharmacies have an opportunity to address suboptimal adult vaccination rates, but many pharmacies lack access to a patient's complete immunisation history; consequently, they are unable to identify which of their patients actually require vaccination. This randomised controlled trial (RCT), called the Immunization Services Model for Adult Rate Improvement (ImmuSMART) study, used an automated telephonic intervention that leveraged such information in an effort to increase rates of vaccination.
ImmuSMART was conducted as a collaboration between the Pharmacy Quality Alliance, Scientific Technologies Corporation, VoicePort, and 246 stores of 3 community pharmacy chains in the US states of New York, Pennsylvania, and Vermont. Over a 1-year period, 21,971 patients with identified vaccine gaps at the participating pharmacies were randomly assigned to receive either usual care or an automated telephonic prompt for pneumococcal and/or herpes zoster vaccines based on patient records contained in state immunisation registries and pharmacy data. According to annual reports produced by the Centers for Disease Control and Prevention (CDC), the records contained in the state immunisation registries (also called immunisation information systems, or IIS) for adults varies by state, with national participation at 44%. During this study of pharmacies in New York, Pennsylvania, and Vermont, adult participation in their state IIS was 19.3%, 48.7%, and 73.7%, respectively.
For intervention patients, a set of automated scripts offering the vaccines under study were developed. The vaccination prompt offered either pneumococcal vaccine, herpes zoster vaccine, or both was appended to the outbound communication that patients were already scheduled. (The nature of these routinely scheduled calls varied by pharmacy chain. Potentially eligible patients were those receiving a medication synchronsation pre-appointment call at 1 chain (100 stores), a refill reminder call at the second chain (88 stores), and a refill ready call at the third chain (58 stores). Patients in the control group received their scheduled outbound communication but without the added vaccination prompt.) Two additional attempts were made if the patient did not answer the phone, if the call went to an answering machine, or if the patient ended the call before receiving the vaccination prompt. Patients who listened to the entire vaccination prompt were asked to give a vocal response indicating their intent to receive the vaccine during their next visit to the pharmacy. If the patient indicated acceptance, a notification appeared within the pharmacy's clinical platform with an alert generated for the pharmacist.
The primary outcome was the proportion with administration of at least one of the vaccines offered between March 2016 and January 2017 based on intention-to-treat principles. Subgroup analyses included vaccination rates by age and sex. An as-treated analysis was also performed.
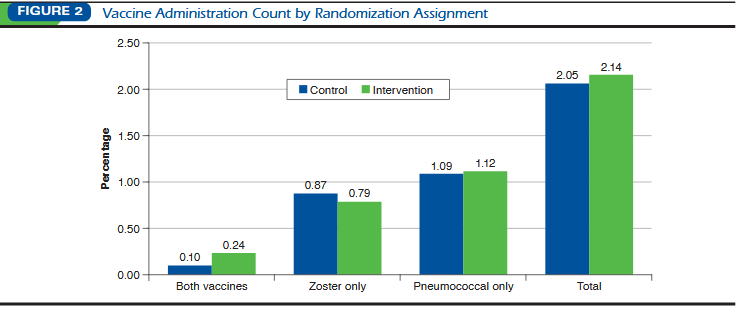
Vaccine administration proportions were 0.0214 (236/11,009) in the intervention group, and 0.0205 (225/10,962) in the control group (odds ratio (OR) = 1.05, 95% confidence interval (CI) = 0.87-1.26). Results did not differ in subgroup analyses based on patient age, sex, or individual pharmacy chain. Among intervention patients, 3,666 (0.333) completed the call by listening to the entire prompt. In an as-treated analysis comparing individuals who completed calls versus control, the intervention increased the odds of vaccination by 26% (OR = 1.26, 95% CI = 1.00-1.61).
Thus, the automated prompt did not significantly increase vaccination rates. Potential barriers included intervention technical flaws, poor adult data in the state IIS, low rates of connecting with patients, insufficient follow-up by the pharmacy, and patients placing a relatively low priority on being vaccinated. Future research could: assess different modalities with stronger potential to reach the patient, such as text and mobile calls, ensure that the technical components integrate meaningfully into workflows, and monitor follow-up from the pharmacy when patients accept vaccinations that are offered.
Journal of Managed Care & Specialty Pharmacy. 2019; 25 (9) : 989-94. https://doi.org/10.18553/jmcp.2019.25.9.989.
- Log in to post comments